Variant prioritisation overview
The Newborn Screening Pipeline aims to maximise positive predictive value of the variants to be reported to the participants. To achieve this in the context of screening for rare conditions in which the prior probability for the baby to have a condition is very low, it is important to keep high specificity (i.e. low number of false positives), while maintaining acceptable sensitivity. As a research programme, the Generation Study takes a conservative approach, with particular focus not to cause harm to families and healthcare system that could be caused by too many false positive findings.
The variant prioritisation and reporting is a two-step approach. Firstly, the automated pipeline is run to prioritise the variants that are most likely to reach pathogenic or likely pathogenic classifications following a set of gene and variant-based filters. Following that, all prioritised variants are manually reviewed, have pathogenicity classifications assigned, and checked whether they satisfy other reporting criteria by a clinical scientist. This section describes variant prioritisation rules applied in the automated pipeline, while manual variant review is covered by the Variant Review SOP.
The schema of variant prioritisation is shown Figure 3. Briefly, the following approaches are used to select candidate variants:
- Variants previously classified as pathogenic or likely pathogenic in the context of conditions included in the screening,
- Variants predicted to cause loss of function of the protein, when this mechanism of pathogenicity is relevant for the screened condition.
- Variants in SMN1 gene identified as pathogenic using targeted callers.
A set of filters is applied to remove potential artefacts, unreliable database entries and variants with known low penetrance or mild phenotype. Lastly, the variants’ genotypes are matched with the expected mode of inheritance (MOI) for the gene.
The rules for filtering variants are specific to each of the potential sources of prioritisation – ClinVar, CVA, internal inclusion list, predicted loss-of-function algorithm or targeted caller. Only variants assigned PASS status in the FILTER column of the appropriate VCF file are considered for prioritisation.
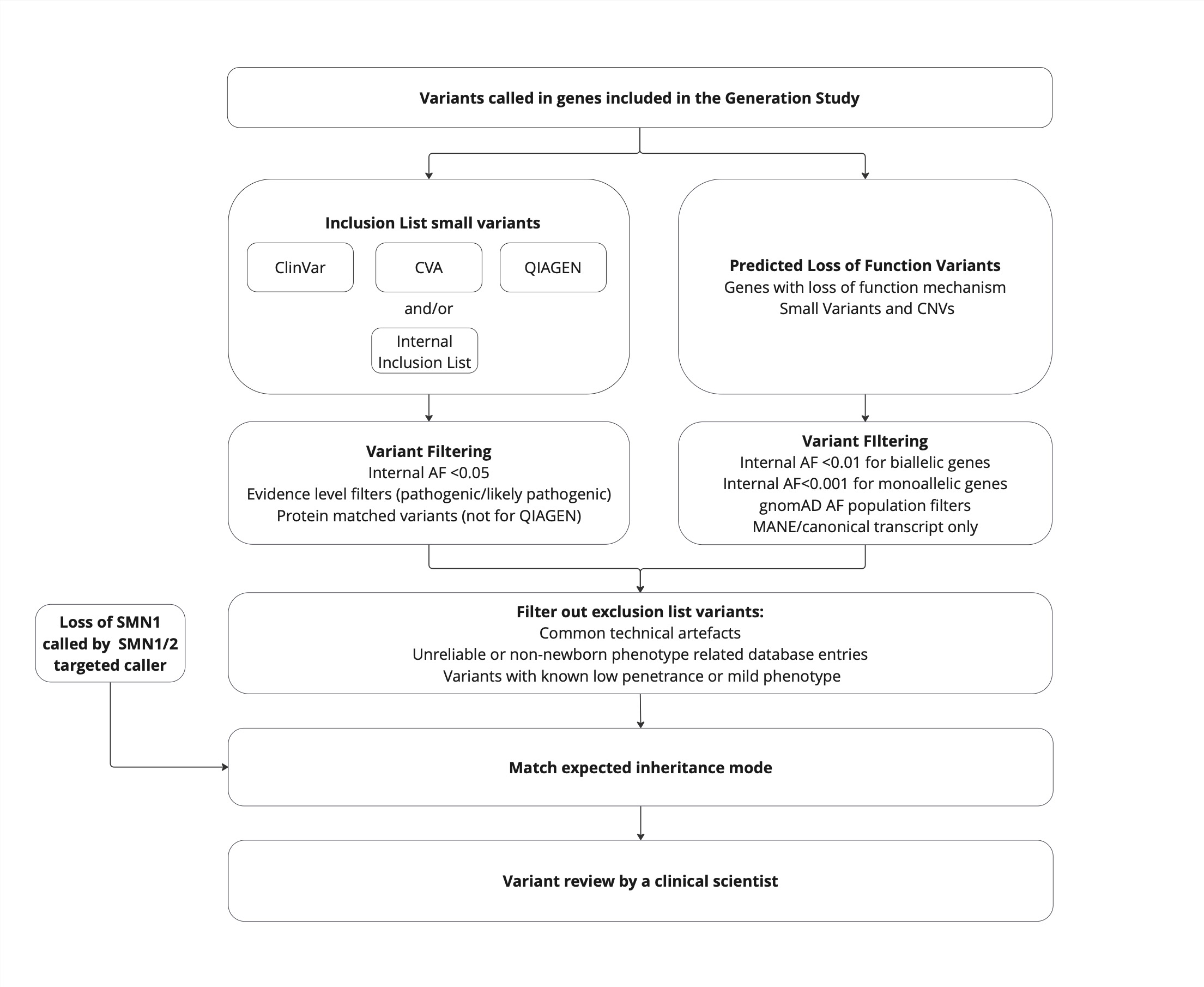
Figure 3: Variant prioritisation overview.
*From Release 12.0 onwards, QIAGEN is no longer used as a source of variant prioritisation.